Intermittent suctioning does not reduce trauma and is less effective. Ultimate responsibility for the treatment of patients and interpretation of these materials lies with the medical practitioner / user. A catheter that is too small may not remove the secretions adequately or result in multiple attempts that can cause trauma to the airway. Please confirm you want to block this member. Reattach any oxygen to the patient if indicated. Infections may result from the possible introduction of bacteria into the respiratory tract if proper suctioning techniques are not performed. If the patient has a fenestrated tracheostomy tube, the unfenestrated inner cannula must be in place before suctioning. To obtain material for analysis of culture. The National Tracheostomy Safety Project has an algorithm for Emergent Tracheostomy Management including cases where the suction catheter is unable to pass. hCL1/k91 The entire tracheostomy tube may need to be changed if replacing the inner cannula still does not allow the suction catheter to pass. Videos are used to aide in learner comprehension of tracheostomy care. There are no absolute contraindications to tracheal suctioning as problems are usually short lived and related to the baseline stability of the patient. The Clinical Consensus Guidelines indicates that the stoma and tracheostomy tube should be suctioned when there is evidence of visual or audible secretions in the airway, suspected airway obstruction, and when the tube is changed or the cuff deflated (Mitchell, 2013). Complications from suctioning are relatively uncommon if performed with care and pre-oxygenation prior to suctioning. Removal of a fenestrated inner cannula with placement of a non-fenestrated inner cannula prevents the suction catheter from passing through the fenestrations, which can cause trauma to the tissue. 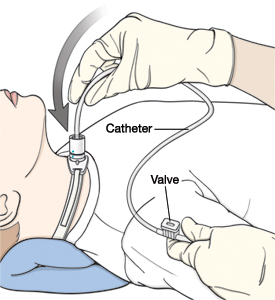
 %PDF-1.2
Airway patency can be checked by attempting suctioning at least every 8 hours. A comparison of open versus closed suctioning in individuals endotracheally intubated showed similar results in safety and effectiveness for rates of mortality and ventilator associated pneumonia (Sola, L & Bonito, S., 2007). Cardiac dysrhythmia from the act of suctioning may disrupt the patients heart rhythm with bradycardia from stimulation of the vagal nerve. prompt assessment by an appropriately trained individual. ?#A5e-sPL8_00L:p5@@uPV[057&[;iwM6o+rBjfT\<0|9>xT67%IR%pG
A>[aA(@ @ H$I8jc\ (^sWz0(>Ul"pR.4IcC;DsH2)3Z@M%*
'P%IHeAbs{c$*ELO.!q9BC$&t9|-$&07bpfKDwJj!GcK~v
;X~O%qgE! @BNsQL$64F>j%GrJc* iPZBN&3
'+3Zgc.AA'H}eS First the inner cannula (if present) should be removed. Art.
%PDF-1.2
Airway patency can be checked by attempting suctioning at least every 8 hours. A comparison of open versus closed suctioning in individuals endotracheally intubated showed similar results in safety and effectiveness for rates of mortality and ventilator associated pneumonia (Sola, L & Bonito, S., 2007). Cardiac dysrhythmia from the act of suctioning may disrupt the patients heart rhythm with bradycardia from stimulation of the vagal nerve. prompt assessment by an appropriately trained individual. ?#A5e-sPL8_00L:p5@@uPV[057&[;iwM6o+rBjfT\<0|9>xT67%IR%pG
A>[aA(@ @ H$I8jc\ (^sWz0(>Ul"pR.4IcC;DsH2)3Z@M%*
'P%IHeAbs{c$*ELO.!q9BC$&t9|-$&07bpfKDwJj!GcK~v
;X~O%qgE! @BNsQL$64F>j%GrJc* iPZBN&3
'+3Zgc.AA'H}eS First the inner cannula (if present) should be removed. Art.  Some individuals are able to project mucous out of the tracheostomy tube by coughing. Patients with tracheostomy are at high risk for preventable adverse events as. Webinar objectives.
Some individuals are able to project mucous out of the tracheostomy tube by coughing. Patients with tracheostomy are at high risk for preventable adverse events as. Webinar objectives.
In cases of acute respiratory distress, where obstruction of the airway or the airway adjunct is suspected, suctioning must be performed emergently, with even minimal preparation. Common ventilator alarms and how to set them and basic weaning from mechanical ventilation will be discussed. Reducing suctioning times to less than 15 seconds can prevent hypoxemia. Suctioning is alifesaving procedure requiring timely and precise methodology. Aa!sa52S1c1H|]/@80@UasR[pI,*;C/v)6a /wlB7,%0H9h}_N8ACSu[BPm!>Q.AA o;vJC J|`D.pOt xu When withdrawing the catheter, continuous suction is applies. Signs of airway obstruction include hypoxia and cardiovascular changes. The opinions expressed are those of the authors. and proper suctioning technique with pressures not exceeding. A tracheostomy tube bypasses the natural humidification and filtration system.
Suctioning should be continuous, not intermittent. Suctioning of the airways should be performed by skilled personnel with appropriatepreparation to prevent. : CD004581. Removal of a fenestrated inner cannula with placement of a non-fenestrated inner cannula prevents the suction catheter from passing through the fenestrations, which can cause trauma to the tissue. Instructor: Terrence Sheffield, RRT-ACCS, RPFT, NPS, AE-C Brief, 10-second suction duration is usually recommended to avoid mucosal damage and prolonged hypoxia. Cough techniques can aid with secretion removal and eventual decannulation. j5( 6h#C9& T`|s u7 a`$',EY0QlQ"6DEy9nF)%xXa!O)H If there is a need for repeated suctioning, care should be taken to maintain and normalize vital signs in between suction episodes with special attention to the heart rate and oxygen saturation levels. Trauma may be prevented through an appropriately sized catheter and proper suctioning technique with pressures not exceeding-150 mmHg (-20kPa). The closed suctions come in two lengths, one for an endotracheal tube and one shorter one specific for patients with tracheostomy. There are no absolute contraindications to suctioning. The National Tracheostomy Safety Project has an algorithm for. Pre-oxygenate the patient with 100% oxygen prior to suctioning to reduce the risk of hypoxemia.
DOI: 10.1002/14651858.CD004581.pub2, The Blom Tracheostomy Tube System (Pulmodyne) is a specialized tracheostomy tube which can allow adults to vocalize either with the cuff inflated or deflated. Inability to pass the suction catheter is a red flag and indicates that the airway is not patent. Higher pressures may result in trauma to the tracheal tissue or hypoxia from aspirating oxygen. Find out information on timing of tracheostomy, swallowing management and communication specific for ALS. A sample interdisciplinary communication form will be provided as well as home care guideline samples. Cuffed versus cuffless tracheostomy. University of Iowa Stead Family Childrens Hospital is part of University of Iowa Hospitals & Clinics.
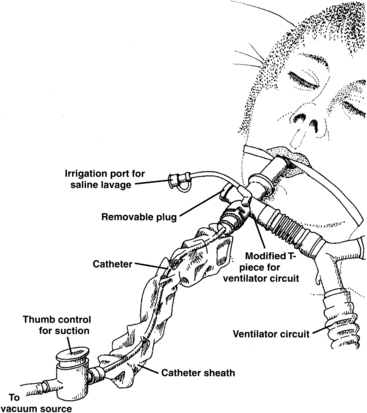
The catheter may also not pass if the tube is dislodged. Hypoxemia can also result from stimulation of the vagal nerve. Please allow a few minutes for this process to complete. [`DaaS#Fsba(#P}]7k5H[^z#6,JaX^(8m!KBM+ ,M,;W 1wJ.0#Lb},d>>`Da/iP5O'wEz d"N@y;L. The tracheostomy effects the normal functions of the upper airway including secretion management and humification due to impaired cough reflex, increased mucous production and impaired actions of the cilia. All Rights Reserved. Even those working with trach tubes for years will likely learn something new in this detail oriented course on trach tubes. resulting in less available oxygen. Risks are associated with suctioning and should be weighed with specific individual patient needs. This. B MocDujeHFq@2u%I@t4an: e1wrMp:+ lra@6#R"ir. +! The amount of secretions varies by patient as does the amount of suctioning needs. Higher pressures may result in trauma to the tracheal tissue or hypoxia from aspirating oxygen. Suction between feedings or discontinue feedings for period of treatment. Once an individual can tolerate a speaking valve or cap, they may be able to cough secretions around the tracheostomy tube, through the upper airway and out of the mouth. Application for continuing education credit has been made to AARC for 1 CRCE. Flush the closed suction tubing with clean water and empty the water receptacle as needed. Adult Tracheostomy Care: Home Edition is a 1 hour recorded webinar which provides information about performing tracheostomy care for adult patients in the home environment. L@ H] RZ2 hp`9FRIpb RI0@0LC*II8D`coSFq t @9V1V The importance of suctioning of both ventilated and non-ventilated patients with tracheostomy cannot be overstated. There is a delicate balance between effectively removing secretions and reducing injury to the tracheal mucosa. Tracheostomy Tubes Webinar: Comparisons and Choices is a 2 hour recorded course that is all about different types of tracheostomy tubes and how to choose the most appropriate tracheostomy tube for your patient. -#?$0)PAM gg,Cu(+ Shallow suctioning is when the suction catheter is passed to the tip of the tracheostomy tube. Suctioning can be anxiety provoking for the patient. Now available! stream Clean hands prior to placing gloves on. fKwHWS[Lz)pb:@Zl`v . Education is a main role of respiratory therapist in the home environment. The catheter should be introduced to the desired depth. Adult Tracheostomy Care: Home Edition Webinar 20% off! Contains spam, fake content or potential malware, Adult Tracheostomy Care Webinar: Home Edition, Tracheostomy Tubes Webinar: Comparisons and Choices, Mechanical Ventilation Webinar: Beginners Guide, Cuffed versus Cuffless Tracheostomy Tubes, Humidification and Hydration for Tracheostomy and/or Mechanical Ventilation, Identify the indications for and complications of a tracheostomy, Note the differences and limitations of tracheostomy care at home During the pandemic it is recommended to use a closed circuit suction to reduce opening the circuit which could result in aerosolizing. Speech-language pathologists may be interested in grasping ventilator information for a whole person approach. Learn about active and passive humidification. Care shouldbe taken to maintain sterility while suctioning the endotracheal/tracheostomy tubes. Please note: This action will also remove this member from your connections and send a report to the site admin. D1#p7# x2 :#6!J`N:97 #pBh,28^|4r3|-l4$ljp2l x6Rp@6 7e)O Xp9 u=\*r8=c7exT8},0Xjn,V$4CRMId~Sf9]%O|/HYeV]Khui&hA(Z$*u:K. Do not add saline unless necessary. The Tracheostomy Tubes Webinar will provide information on patient candidacy for the types of tubes. Blood stained secretions may indicate tracheal injury. Tracheal suctioning is performed to remove secretions from the tracheostomy tube and airway in order to maintain a patent airway and avoid tracheostomy tube blockages. Occlude the suction port with a gloved thumb and suction upon removal of the catheter. If the need for CPT is documented, it must be ordered by a physician describing the area to be treated and the frequency of treatments. Suctioning is an important part of care for both the individual with tracheostomy as well as laryngectomy. It is difficult to discern the exact reason. Suction pressure should not exceed -150 mmHg (-20kPa) and is appropriate for most patients. The decision for tracheostomy placement for a person with ALS is personal. Percutaneous placement of central venous catheters, Abbreviations commonly used in the nursery, Percutaneous placement of central venous catheters, Technique for insertion of a pericardial tube, Technique for insertion of an endotracheal (ET) tube, Iowa Neonatology Handbook: Authors and contributing authors, Translations of the Iowa Neonatology Handbook, University of Iowa Indigenous Land Acknowledgement. Review the different types of speaking valves and benefits for those with tracheostomy and mechanical ventilation: Passy-Muir, Shiley, Shikani, and Montgomery. Blood stained secretions may indicate tracheal injury. eliminating the need to disconnect the individual from the ventilator. Anxiety can be associated with suctioning. The instructor will explain the relationship between compliance and resistance and provide information on different pressures related to mechanical ventilation regarding lung mechanics (PIP, pleateu pressure, transpulmonary pressures, mean airway pressures). Iowa Neonatology Fellows Larger catheters may cause damage or occlude the tube resulting in hypoxia. Do not apply suctioning while introducing the catheter as this can increase the risk of mucosal damage and hypoxemia. Tracheal damage and hypoxia can also be minimized by using an appropriately sized suction catheter. Auscultate chest prior to suctioning. Copyright 2022 The University of Iowa. If the suction catheter is passed further than the end of the tracheostomy tube, this is considered deep suctioning. Hypoxemia may result as some oxygen provided to the patient may be taken from the vacuum created during suctioning, O2 therapy wall flow meter/portable bottle and tracheostomy mask, Personal protective equipment (gloves, gown as needed, ideally goggles/mask).
Suction should not be applied while the catheter is being inserted down the ET tube. Once a need for tracheal suction has been established, the careprovider should make sure all equipment is available and functioning adequately. @D3 @ZD2//:LhlSEqytC#;#KY,l2Y*/j,${Fl The tip of the suction catheter will not be inserted beyond the end of the tube. The amount of suction applied to the catheter should be between 40-80 mmHg. It is recommended that the external diameter of the suction catheter to be no more than half of the internal diameter of the tracheostomy tube. /Length 10 0 R Open suction catheters involve using singe-use catheters. Tracheostomy and feeding tubes are often placed concurrently. Vibration and percussion (CPT) will not be performed routinely prior to suctioning. versus acute care, Demonstrate how to perform trach care (inner cannula changes, site Atelectasis can occur as the alveoli may close and be unavailable for gas exchange. An individual who is awake and cooperative may be asked to cough up secretions in order to limit suctioning and potential tracheal trauma. Large quantities of blood or persistent bleeding should be investigated to determine the cause of the bleeding. Closed suctioning consists of a catheter enclosed in an outer plastic sheathe which allows the same catheter to be used multiple times. Large quantities of blood should be investigated as to the cause of the bleeding. An obstruction of the tracheostomy tube may be due to thick secretions or blood. If the patient has a fenestrated tracheostomy tube, the unfenestrated inner cannula must be in place before suctioning. Prior to beginning the procedure, educate and explain the suctioning procedure to the patient. Following suctioning, ventilate the infant with an FiO2 no greater than 0.10 above that used prior to suctioning. Suctioning should be continuous, not intermittent. A cuffed and non-fenestrated tracheostomy tube should be used for COVID positive patients or suspected patients. Closed suction catheters are usually changed every 72 hours or according to manufacturer instructions. Although tracheostomy tube changes are relatively simple and easy procedures, it should only be changed by someone who is trained and competent to do so. There is no clear consensus on how frequently an individual should be suctioned. Course is coming soon! An apron should be worn to protect clothing and other patients. Closed suctions add weight to the ventilator circuit. If done appropriately with caution, it decreases the risk of infection, pooling of secretions, and prolonged hypoxia. There is a delicate balance between effectively removing secretions and reducing injury to the tracheal mucosa. Multidisciplinary tracheostomy teams have been shown to improve outcomes for patients with tracheostomy. Subirana M, Sol I, Benito S. Closed tracheal suction systems versus open tracheal suction systems for mechanically ventilated adult patients. iR@WtQ'THLBpn ungyZ0wV;*) A t[SX1_,6tf|d=U0] ++z- x)0y Be!FGCEe> Peer Review Status: Internally Peer Reviewed. Easy passage of a suction catheter and removal of secretions confirms proper placement and patency of the tracheostomy tube. care, cuff management, suctioning), Identify the steps for tracheostomy tube changes. The procedure should not take longer than 10 seconds. Support the patient in a position that will facilitate coughing (unless contraindicated). Suction pressure should not exceed -150 mmHg (-20kPa) and is appropriate for most patients. For effective deep suctioning, many experts advocate advancing the suction catheter until the carina, where resistance is met.
The ability to forcibly cough secretions through the upper airway is one indicator for readiness of decannulation. Remove a fenestrated inner cannula and replace with nonfenestrated inner cannula prior to suctioning. Some inner cannulas must be reinserted before connecting to the ventilator circuit. The adequacy of suctioning can be assessed by the clearance of secretions, improved breath sounds, improved air entry, good pulse oximetry readings, and improvement in respiratory distress in a patient. In this course, the risk of inappropriate tracheostomy tubes based on the size and length will be provided. Saline may be used if the infant has thick tenacious secretions which cannot be extracted by using suctioning alone. If there was an inner cannula and it was removed, replace it with a clean inner cannula. Suctioning with a fenestrated inner cannula may allow the catheter to pass out of the fenestration, leading to possible damage to the posterior tracheal wall. Tracheal suctioning can be performed either with open circuit or closed circuit (Ballard) suctioning. This is a red flag and requires quick attention. In-line suctioning preferred for indications other than obtaining material for culture.